In March of 2024, the Vancouver Divisions Seniors and Frail Elder Committee partnered with the Vancouver Primary Care Networks to deliver an information session for Primary Care Providers to share valuable information to help them support their frail senior patients. 81 Primary Care Providers attended the session, which was a follow up from the PCN Engagement Forums held in November of 2023, where we engaged providers on the barriers they experience when trying to support their frail senior patients to live well in the community. At the information session, attendees received presentations from the PCN Interprofessional Team and Vancouver Coastal Health Vancouver Community Services, as well as several Community Partner Organizations, on the services they provide to support frail seniors living in the community. Case studies were used to support more practical takeaways.
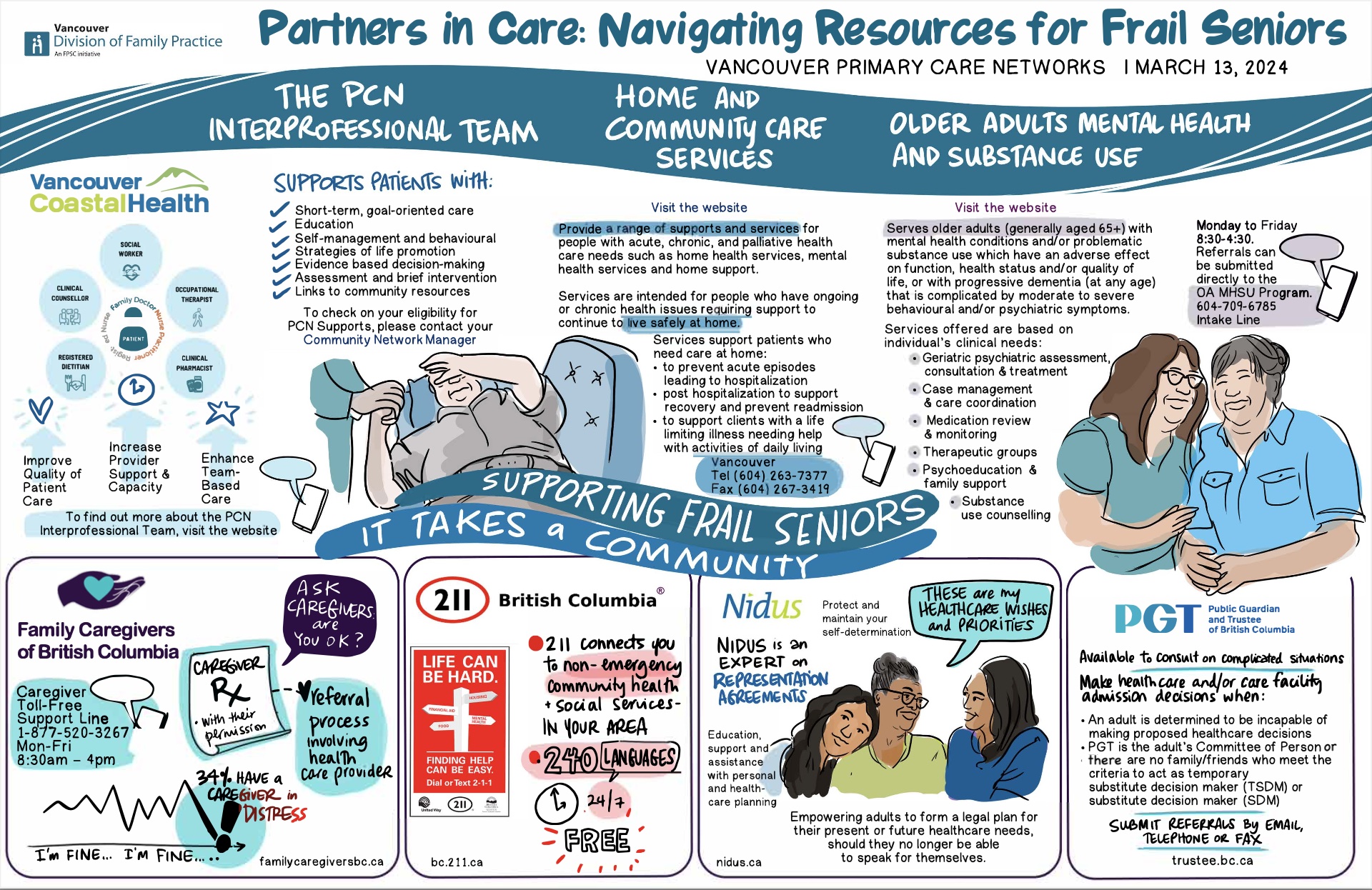
The infographic below gives a high level summary of the event.
Event Recordings
Did you miss the event, or need a refresher? You can view the recorded presentations for the event below.
- PCN Interprofessional Team (IPT) Presentation
- VCH Vancouver Community Services Presentation
- Family Caregivers of BC Presentation
- 211 BC Presentation
- Nidus Presentation
- Public Guardian & Trustee Presentation
Event Resources
Did you miss the event, or need a refresher? You can view and download the resources below including the presentation slides and the Patient Journey Maps from the case studies shared at the event.
Q & A
Many different disciplines work together within Home Health Services to support patients. Depending on the patient’s needs, they could be first connected to a Case Manager, a Nurse, an Occupational Therapist, a Physiotherapist, a Social Worker, a Dietitian, a Speech Language Therapist or a Spiritual Health Practitioner. Depending on the needs of the patient, these clinicians may refer on to other programs such as Adult Day Programs, Long Term Care, or Home Support Services.
You can find a recently updated Home Health referral form on Pathways (Look up Home Health Care in Health Authority Services). On this form, describe the needs of the patient in detail, and then the intake team will review and determine what’s the best first discipline to provide an initial assessment. It could be an Occupational Therapist to do an assessment of safety in the home. It could be a Home Care Nurse that is coming in to do a follow up to wound care, or a Case Manager who is doing assessments related to accessing other services or initiating a longitudinal home support strategy for the patient.
Yes, these are separate programs that are targeting two different sets/levels of needs across the continuum. They have different eligibility requirements and referral pathways – meaning separate referral forms and intake processes. The PCN IPT supports mild to moderate needs that can be supported in a limited amount of sessions. They do mostly virtual appointments, with options for in-person appointments at two locations in Vancouver. The updated Home Health Referral Form can be found on Pathways (Look up Home Health Care in Health Authority services). For the IPT Referral Form, please contact pcn@vancouverdivision.com.
Within each of these programs, the OTs are supporting a different level of need. For example, PCN IPT OTs do not do home visits, although they do see patients in person at our two IPT Hub locations in Vancouver (George Pearson Centre or Three Bridges) depending on the patients needs. The PCN IPT OTs are more focused on things like energy management, sleep, space, setting up schedules, etc. They also work collaboratively with other members of the PCN IPT (Clinical Counsellors, Social Workers, Registered Dietitians, Clinical Pharmacists) to set smart goals for people. They focus on mild to moderate, short-term needs. If a patient needs support in their home, such as equipment assessments, or functional or safety support then that is more of a Home Health pathway.
Within Home Health Services, we have one referral pathway for Home Health Services, and a different referral pathway for Older Adult Mental Health & Substance use. Within both of these pathways, intake teams are doing clinical assessments and risk ratings to determine urgency. If something is very urgent, they are going to prioritize that visit, possibly within 48 hours. If it is less urgent it may be a week to two weeks.
For the PCN IPT, if clinics have access to this program, they make a referral through the referral form which can be embedded into the clinic’s EMR. As these services are more mild to moderate, and typically non-urgent, there is a slower turnaround time for these services. Depending on the discipline and need, it can take 3 – 4 weeks to up to 10 weeks.
Home Vive is a primary care program for very, very frail people who cannot leave their homes to access care. Primary Care Providers, Nurses and Social Workers function as a team to support these patients. Home and Community Care is interested in looking at other ways of linking up primary care with Home Health Services. We have launched different initiatives, such as the Personalized Support & Stabilization Service – this is a team of Nurse Practitioners, Nurses and rehab staff that support frail elders who have come to hospital and need more intensive rehab and medical stabilization back at home. The goal is to get people home as soon as possible.
For the Older Adult Mental Health & Substance Use services, we do have very complex clients with complex needs that are both psychiatric and medical. Because of that, we have a Geriatrician who supports our program. There are some other pockets in Home Health where Geriatricians are doing outreach, but it is very limited. It is something that we would certainly like to have in the future because it is a growing need with people living longer.
We have done some redesigning in our program to hit some better targets with the growing older population. We are using a triage tool and much like Home Health intake, it depends on the acuity of the client. We have clinicians that are able to reach out within 48 hours to the highest acuity. This can look different depending on our physician availability. Our Psychiatrist can also be triaged for acuity. It could be as quickly as a couple of days to a couple of weeks depending on the need. It is really helpful for that triage when risk and acuity are communicated.
Within the PCN IPT, we do have clinicians who have a variety of language skills. This is not by design, but we do take advantage of this as we can. We also have access as part of VCH to Provincial Language Services (PLS) telephone interpretation. All VCH Programs (including Home Health Services) can access these interpretation services.
You can refer your patient using the Home Health Services referral form and indicate you are interested in an Adult Day Program. Patients and their caregivers can also call the VCH Central Intake line (604-263-7377) to initiate a referral. We are working across our teams to look at how we can expedite those referrals. We are keen to support the Adult Day Programs to open up as many spaces as possible, and we know we currently have some spaces in Vancouver. We know these programs are of huge benefit to patients and their family members.
The reality is that we have to be very creative with how services are organized to meet the demand and reach as many people as we can. We have many strategies to recruit community health workers, who are the pillars of the system. We need to continue to value these roles and encourage people to pursue them. We cluster them to try to be more flexible and keep people within neighborhoods or buildings. But they still have limited time. We are also looking at how to support transportation for these roles as well.
We do know that people want and would benefit from that consistent care from a familiar community health worker, but there are lots of things to navigate in terms of scheduling. Scheduling of staff is an important consideration for clients during triage, but it is also logistically challenging, especially in a human resource crisis. We have made some innovations with scheduling i.e. clusters and neighborhoods to support improved consistency.
No it is not. Although people usually have a family member or friend who can offer translation support. For the Registry, people can upload anything, in whatever language they choose, but the form fields, instructions and tips are in English.
When people register their documents, they give permissions to consent to who has access. In some cases, the Public Guardian and Trustee has the right to access information without consent as well.
The Public Guardian and Trustee will use the registry to determine whether there is a Representation Agreement.
The Personal Planning Resource Center part of the website is operated by a non-profit charitable organization. The NIDUS Registry site is operated by the NIDUS personal Planning Resource Centre – so it is community based. The database is managed by a technology company who are experts in the field with the highest privacy measures. We have Privacy Consultants who support this. The database is held in BC.
The information that PGT might be interested in would support us to get to know the patient’s health needs better – so basic demographic information, and any proposed healthcare treatment, has there been a determination of incapability, and does the healthcare provider feel there is anyone else that should be involved. Our regional consultants would then follow up with a phone call with the healthcare provider to learn more details.
There are lots of different types of legal authorities. Power of Attorney allows the designate to support financial and legal decision making. It doesn’t necessarily mean they are authorized to make healthcare decisions. If a Substitute Decision Maker is contacted to make decisions about a person’s healthcare, that authority doesn’t carry over to any other parts of the person’s life. They would only be consulted for the current healthcare treatment that the healthcare provider is looking to get consent for.
There is a criteria to assign a Temporary Substitute Decision Maker – for example you have to be an adult, you have to have contact with the patient within the last year, you cannot have a known dispute with them and willing to comply to the duties, etc. As a healthcare provider, you are looking to see if the Temporary or Substitute Decision Maker meets the criteria and if not, you move down the list. If there is no one on the list who meets the criteria, that’s when the PGT might be contacted.